80 year old female with shortness of breath
Long case
1701006104
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box
CONSENT : An informed consent has been taken from the patient in the presence of the family attenders and other witnesses as well and the document has been conserved securely for future references.
1701006104
CASE
My case is of 80 year old female ,home maker by occupation ,came to casualty with complaint of shortness of breath since 10 days .
HISTORY OF PRESENT ILLNESS
Patient was apparently asymptomatic 20 years back , then she developed headache which is insidious in onset and gradually progressive ,she also had giddiness , initially used some herbs but symptoms didn't subside,so went to local hospital and she was diagnosed of hypertension ,and was prescribed medication.
Currently she is on tab.Atenlol 50 mg+ Amlodipine 5 mg daily
15 yrs back she had history of excessive urination and thirst for which she went to local hospital and diagnosed as diabetic and was prescribed Tab.metformin 500 mg once daily.
3 years back,she developed shortness of breath ,which was insidious in onset initially during activity ,but later progressed to even at rest.
She was admitted in a local hospital and treated ,and was discharged after 1 week .
2 years back ,she had similar episode of shortness of breath ,and bilateral pedal edema, pitting type ,so went to hospital again and was discharged after 1 week.
10 days back ,she again developed shortness of breath ,which is insidious in onset gradually progressive initially on exertion and later even on rest
She also had dry cough which was insidious in onset and gradually progressive.
She also had chest pain , which was aggravated on coughing .
Pateint also has complaints of orthopnoea and paroxysmal nocturnal dypsnoea
Effect of illness on her daily activities
Initially she used to work in fields ,and do household works in herself ,but due to shortness of breath she is unable to do regular daily activities .



PAST HISTORY
Medical history
Known case of hypertension since 20 years on medication
Known case of diabetes since 15 years on medication .
Past Surgical history
Appendictoemy 3 yrs back
FAMILY HISTORY:-
Not significant.
PERSONAL HISTORY
Diet -mixed
Apetite- Decreased
Bowel and bladder - Regular
Sleep -adequate
Addictions - no addictions
GENERAL EXAMINATION:-
Patient is conscious ,coherent, cooperative
Well oriented to time ,place ,person .
Moderate built and moderately nourished.
Pallor - present
Cyanosis - absent
Clubbing - absent
Icterus - absent
Lymphadenopathy- absent
VITALS
Bp -140/70 mm of hg
PR -52 bpm, irregularly irregular
RR - 26 cpm
Spo2- 84% on room air ,96% on oxygen(4 Lt)

SYSTEMIC EXAMINATION
CARDIOVASCULAR SYSTEM
INSPECTION
Shape of chest- elliptical , bilaterally symmetrical
JVP- raised at the time of admission
Apical impulse - present
No precardial bulge
No engorged veins
No visible scars and sinuses
Other pulsations
Carotid pulsations are visible in the neck
Link
PALPATION
All the Inspectory findings are confirmed
Apex beat -1cm lateral to mid clavicular line on left side
No thrills
PERCUSSION
Both right and left heart borders are normal
AUSCULTATION
Heart sounds - both S1 and S2 are heard
No murmurs
RESPIRATORY EXAMINATION
INSPECTION
Trachea - central in position
Shape of chest - elliptical , bilaterally symmetrical
Movements of chest - equal on both sides
Apex beat - 1 cm lateral to midclavicular line on left side
PALPATION
All the inspectory findings are confirmed
No tenderness
No local rise of temperature
PERCUSSION
Resonant note over the lung
AUSCULTATION
Breath sounds - vesicular
Basal crepts are present
No wheeze
ABDOMINAL EXAMINATION
INSPECTION
Shape of the abdomen- flat
Umbilicus - central in position
Abdominal movements - normal with respiration
No visible scars,pulsations
No engorged veins
PALPATION
All the inspectory findings are confirmed
No abdominal tenderness
No local rise of temperature
No guarding and rigidity
No fluid thrill
Liver - palpable 2 cms below costal margin
Spleen - not palpable
PERCUSSION
No free fluid
AUSCULTATION
Bowel sounds heard
CENTRAL NERVOUS SYSTEM EXAMINATION
Patient is conscious ,coherent and cooperative
Oriented to time ,place and person
Memory - immediate , short term and long term memory are assessed and are normal
Language and speech are normal
Gait - normal
SENSORY EXAMINATION
Touch - felt on both right and left side
Pressure - felt on both right and left side
Pain - felt on both right and left side
Temparature - felt on both right and left side
Vibration - felt on both right and left side
MOTOR EXAMINATION

Reflexes - normal
INVESTIGATIONS
COMPLETE BLOOD PICTURE
Haemoglobin - 5.5 gm / dl
TLC - 7400
Platelet count - 2.88 lakh/cu .mm
PCV - 19
MCV - 63
MCHC - 18
Peripheral smear - microcytic ,hypochromic cells are seen

LIVER FUNCTION TESTS
Total bilirubin - 1.05
Direct bilirubin - 0.31
AST ,ALT - normal
ALP - normal
Albumin - 3.68
RENAL FUNCTION TESTS
Urea - 46
Creatine - 1.1
ESR :normal
Reticulocyte count - 0.5
Sr. Iron - 49mg/dL
Na+ - 129meq/l
cl. - 102meq/l
k+ 3.6meq/l
Mg- 1.7meq/l
CHEST XRAY

USG

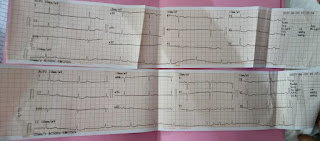
ECG
2d echo:-

Comments
Post a Comment